We've provided you with three reports that enable you to audit file access at three levels: by patient, by user and by clinic. Below is a description of each of these reports.
- Liste des consultations et consentement pour un patient
- Liste des dossiers consultés par un utilisateur
- Liste des accès suspicieux par clinique
To access these reports, please follow these steps: Generate a report
⚠️ Information Access Rules
- The reports below provide the consultations and consents of users with whom you are exchanging an active mandate (received mandate or issued mandate).
- Only consultations and consents from the login institution from which the report is generated are displayed in the report.
- The administrator account holder can view the consultations and consents of all users with a mandate in their login institution.
Liste des consultations et consentement pour un patient Report
Goal - List all the consultations made and all the consents that have been taken of a patient's file related to the mandates of the user generating the report.
Application field - Indicate the number of the file beforehand (8 digits in total). If your number has only 3 digits, please add as many 0 as you need until a total of 8 digits (for example, 348 should be 00000348).
Timelapse - The report generates all the consultations and the taken consents for the active mandates as of today.
Displayed information
This is all the information shown for each patient:
- Patient's general information: the number of the patient's file, last name and first name, health insurance number (HIN), date of birth, and sex.
- History of ad hoc consents (users who clicked on the consent button to display all the contents of the file):
- The name of the user who took the consent of the patient's file and the Omnimed user's ID.
- Name of the person on whose behalf the specific consent is taken.
- Date and time of the consent that has been taken (24h format).
- Please note that the type of consent GMF is not listed.
- If the page is blank, it means that no consent has been taken.
- History of consultations (users who accessed the patient's file):
- If the column Created by is empty, it means that it is the user of the second column who has entered or has taken action in the file on its name.
- If the columns Created by and On behalf of are displaying names, it means it is the user of the column Created by that has entered or taken action in the file on the name of the column called On the behalf of.
- The date and time of the consultation (24h format). For example, if the patient file is accessed at 8:01 and action is saved at 8:15, you'll see 8:01 on the report.
- The reason for the consultation* (The title of the clinical note typed down during the consultation). If this field is empty, it means that there is no title or no edited clinical note.
- The type of the clinical note (contact type): clinical visit, inbound ou updated information. If this field is empty, it means there is no information available.
Liste des dossiers consultés par un utilisateur Report
Goal - List all the viewed files and edited clinical notes related to the same file for a given user in your institution.
Application field - Predetermine a user. It is only possible to generate the report for the users of the institutions to which the person who is executing the report has access.
Timelapse - The report generates all the consulted files by the given user for the period of the mandate that binds the user to the person who ran the report.
Displayed information
For each consulted file, here's the information listed:
- The patient file number, first and family names, health insurance number (HIN), date of birth, sex, and date of the viewed file.
- The date of access to the file.
- Reason for consultation* (the title of the edited clinical note during consultation). If the field is empty, it means there is no title or no clinical note.
- Taking consent - If consent is taken (X in the consent field if the consent has been taken by the user). If the field is empty, it means no consent has been taken.
⚠️ The empty field Reason of consultation means that there is no clinical note, which is a visualization or added information within the summary. To verify this information for a specific date, enter the patient's file in the EMR, click on the locked eye at the top right corner of List of clinical notes and select the given date. Open the note to see the content section of the note listing all the actions that have been done on this very note. It is also possible to consult the history of the clinical note from the Clinical note's visualization.
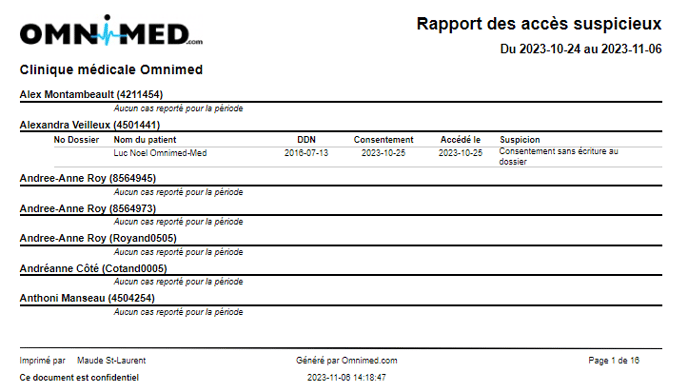
Liste des accès suspicieux par clinique
Goal - To list suspicious record accesses by users at your institution. More specifically, the report identifies cases where a user has accessed:
- their own record;
- a colleague's record;
- a patient's record with the same family name;
- a record where consent has been taken but no writing has been made (i.e. no clinical note, no task, no prescription, no result, etc.).
Application field - The report displays all users who have given or received a mandate in the institution for the selected time period.
Timelapse - Select a time interval. The report generates all consulted records meeting the above criteria by the clinic's users for the selected period.
Displayed information
For each consulted file, here's the information listed:
- Time interval applied to report;
- Name of institution;
- Name and Omnimed ID of users;
- Patient file number;
- Patient name;
- Patient's date of birth;
- Date of consent (if applicable);
- Date of access to record by user;
- Reason for suspicion.